



















Rationalising prescribing of unlicensed specials to children
European Statement
Clinical Pharmacy Services
Author(s)
Helen Cooper, Sheatha Abumehdi
Why was it done?
A lack of licensed formulations for children means that use of unlicensed and off-label medicines is often the only appropriate alternative [1]. Local prescribing data demonstrates wide variability in concentrations of unlicensed specials supplied, at significant cost. This project aims to standardise medicines prescribing for children, improve patient safety by reducing inadvertent dose misadministration due to varying concentrations, reduce spend, and improve the effectiveness of working relationships between hospital and community healthcare teams.
What was done?
Prescribing and procurement data were used to analyse, review and harmonise paediatric prescribing practices in a UK clinical commissioning group, with focus on rationalising use of unlicensed specials.
How was it done?
A target list of ten medicines was identified, based on variability of strengths and formulations available, and cost. A team of two dedicated specialist paediatric hospital pharmacists was funded to set out strategies to standardise prescribing of those target medicines, and to improve understanding of prescribing and supply of unlicensed medicines to children. Various methods were used, including; email communications advertising the roles and support offered; establishing a Paediatric Formulary Group; promoting the local Paediatric Formulary; creating paediatric prescribing pathways; reviewing specials prescribing and supporting switches to alternative formulations; and delivering a paediatric prescribing webinar.
What has been achieved?
Reviews of specials prescribing were initially undertaken in two of the six boroughs in the region. 138 switches to a preferred formulation for safety and/or cost-effectiveness were identified and discussed between July-October 2021. Risks associated with prescribing multiple concentrations of liquid medicines were identified and measures were put in place to prevent patient harm. The webinar was well attended, and although it cannot be quantified, awareness of the Paediatric Formulary has improved. The project is on-going and at this time the impact on spend cannot be shown but will be reported later this year.
What next?
The specific knowledge and skills of specialist paediatric hospital pharmacists are highly valuable in driving specials medicines rationalisation for children in the community. Future plans for expanding the project include extending the service to other boroughs in the region and widening the target list of medicines.
References: 1.Rawlence E et al. Is the provision of paediatric oral liquid unlicensed medicines safe? Arch Dis Child Educ Pract Ed. 2018;103(6):310-3. 2.Neonatal and Paediatric Pharmacists Group. Position Statement 18-01 Using Standardised Strengths of Unlicensed Liquid Medicines in Children. Version 5, April 2020.
How to be in friendzone: geriatric and pharmacy ?
European Statement
Clinical Pharmacy Services
Author(s)
François TISSERAND, Pierre MENAGER, Alexandre NAVID, Léa ROUSSET, Adeline BANNIER, Julie MORIO, Hélène PERRIER, Elsa JOUHANNEAU
Why was it done?
The geriatricians contacted the pharmacy to deliver training courses to the geriatric residents. This has enabled pharmacists to develop a close relationship with geriatricians to offer them clinical pharmacy activities in their ward. Geriatricians were familiar with clinical pharmacy, in particular the medication reconciliation, which is used to perform the former in other hospitals. Geriatricians are concerned with iatrogenic illness and therefore see medication reconciliation and pharmaceutical analysis as a relevant approach to clinical pharmacy.
What was done?
A successful model of partnership between Geriatrics and Pharmacy has been created and developed.
How was it done?
A first meeting was held between geriatricians and pharmacists. It was decided a pharmacy resident would be dedicated to a given geriatrician. This first resident’s objectives are to follow the medical rounds and to carry out medication reconciliations upon admission and discharge. Pharmaceutical support has enabled real-time validation for the prescription of the appropriate drugs. As the internship progressed, the resident became the privileged interlocutor for a Pharmacy-Unit relationship.
What has been achieved?
To date, 37 medication reconciliations were carried out, where the resident followed 2 medical rounds per week over 17 weeks. All unintentional discrepancies were corrected (n=13). Concerning the appropriateness of prescriptions, 16 inappropriate medications were stopped. During the medical rounds, 34% of the therapeutic problems (n=35) were related to inappropriate drug according to guidelines, 17% to dosing errors, 14% to drugs without indication. More than 50% of pharmaceutical interventions were judged capable of preventing harm that requires increased monitoring or treatment or lengthening of the hospital stay (63%). During this period, 54 questions were asked and discussed between the resident and the geriatrician to improve patient care. At the geriatricians’ request, two courses were organized about non mastered topics. On the ward, the resident acted as a go-between for a number of issues such as referencing medical devices, rearranging the storage of medicines or finding the right contact person for information activities.
What next?
What has been done needs to be continued and improved. A pharmacist-geriatrician cross-training should be implemented soon. New activities with pharmacist-geriatrician interactions are being created, such as day hospitalization for falls in the elderly population and a geriatric emergency unit.
Evaluation of pharmacist-provided medication therapy management service on reducing unplanned readmissions in adult patients in Singapore
European Statement
Patient Safety and Quality Assurance
Author(s)
Elena Lee, Yue Feng Toh, Nathaniel Lim
Why was it done?
Older patients on polypharmacy are predisposed to drug related problems (DRPs). While MTM service with pharmacist involvement can reduce DRP occurrence, few have examined its impact on reducing unplanned readmissions.
What was done?
This study was designed to determine whether a pharmacist-provided medication therapy management (MTM) service can reduce unplanned readmissions through the comparison with patients receiving usual care.
How was it done?
A retrospective cohort study was conducted in Changi General Hospital. Patients present for MTM service from Jan 2016 to Dec 2019 were included in the intervention arm (n=96) while patients who attended specialist outpatient clinics were recruited as control (n=98). Index visits from the same patient within 6 months of an earlier visit were excluded. Primary outcome was the change of unplanned admission post and pre 6-month of index visit comparing intervention arm against control arm. Secondary outcomes were descriptive of DRPs identified, number of recommendations from pharmacists, types of interventions and the potential risks avoided. Primary outcome analysis was conducted with linear regression and adjusted for potential confounders.
What has been achieved?
MTM sessions resulted in the reduction of unplanned admission rate by 0.83 (95% CI: -1.31, -0.34), p=0.001, after adjusting for confounders. For patients with admission prior to the index visit, the intervention arm had statistically significant lower incidence of unplanned admission post and pre 6-month of index visit by 0.916 as compared to control group (p=0.018). There are higher number of DRPs (144 vs 2) and pharmacist recommendations (40 vs 2) were found in the intervention arm compared to control arm respectively. The most prevalent types of DRPs were ‘Non-adherence’ (80.6%), ‘Drug omission’ (5.6%), and ‘Inappropriate dose’ (2.8%). The most common potential risks avoided were increased cardiovascular risk, n=29 (22.1%), increased fall risk, n=18 (13.7%) and increased risk of fractures, n=17 (13.0%).
What next?
The study suggests that pharmacist-provided MTM service decreased unplanned readmission rate. It has improved medication safety and quality of care by identifying and resolving more DRPs.
EXPERIENCE OF PATISIRAN OPTIMIZATION BUILDING HEALTHCARE TEAM
European Statement
Clinical Pharmacy Services
Author(s)
CRISTINA GONZALEZ PEREZ, LUCIA GALÁN DAVILA, MARTA ORTIZ PICA, ELENA GARCIA SUAREZ, MARIA MOLINERO MUÑOZ, LIDIA YBAÑEZ GARCIA, NATALIA SANCHE-OCAÑA MARTIN, MARIA DE LA TORRE ORTIZ, JAVIER CORAZON VILLANUEVA, JOSE MANUEL MARTINEZ SESMERO
Why was it done?
Our hospital is a reference in our community for this rare disease. Since patisiran was approved, we have treated 19 patients. Due to the high cost of patisiran and the few patients treated, it is necessary to optimize patient treatments in the most efficient way.
What was done?
Transthyretin (TTR) amyloidosis is a rare disease caused by mutations in the TTR gene. These mutations alter the normal function of TTR protein, creating slowly progressive condition characterized by the buildup of abnormal deposits of amyloid in body’s organs and tissues.
Patisiran is a TTR specific small interfering RNA (siRNA) formulation in lipid nanoparticles, which has been shown to substantially reduce the production of abnormal TTR in patients with hereditary amyloidosis TTR.
With this project we look for achieve the greatest possible savings from patisiran drug without affecting the patient’s efficacy.
How was it done?
We created a working group with neurology department, to define patient’s groups according to:
– Prescribed doses (doses per patient weight; 0.3 mg/kg).
– Preparation’s losses because of the filters
– Losses of the extraction process.
– Other individual conditions as posology or personal preferences.
Patients belonging to the same group have to administrate patisiran the same days.
As the patient’s weight can change along the time, we agree with doctors and nurses to weight the patients every six months to perform doses adjustments. Therefore, every six months we should regroup the patients to optimize the most.
What has been achieved?
These clusters have made possible to reduce wasting vials and therefore to permit significant savings. We estimate around 208.115 € savings/year.
What next?
With this practice we look for a more efficient and sustainable rational health system. The savings achieved can be used to treat other patients or promote new investigations. Also, it makes possible a better healthcare team performance, working together for a better attention, health quality, security, and treatments efficiency. Monitoring weights to adjust doses and closer follow-up of patients by the different members of the multidisciplinary team are examples of the achievements.
Initial observations on the implementation of a clinical pharmacy service in a rural hospital in Austria
European Statement
Clinical Pharmacy Services
Author(s)
Sonja Guntschnig, Aaron Courtenay, Ahmed Abuelhana, Michael Scott
Why was it done?
The service was established as part of the implementation of a new pharmacy into the hospital. The aim of this good practice initiative was to introduce multidisciplinary work on the wards and provide clinical pharmacy support for the ward personnel. Furthermore, it determined what types of clinical pharmacy interventions are needed at a rural 360-bed hospital in Austria, and assessed the physicians’ acceptance rate of the pharmacists’ suggestions.
What was done?
A new clinical pharmacy service (CPS) was introduced into Tauernklinikum Zell am See.
How was it done?
Data on 550 interventions made by one clinical pharmacist were collected by convenience sampling over a one-year period and rated on a six-point clinical significance scale. A subset of 26 interventions was rated for clinical significance by four independent physicians to determine inter-rater reliability (IRR). A two-way model inter-rater reliability analysis was performed for the four different physician assessments using SPSS to determine intra-class correlation (ICC).
What has been achieved?
Prompt acceptance rate by the physicians involved was 71.3% (392/550). In 26.9% (148/550) of all cases, the physician considered a change. The overall average score for all 550 clinical pharmaceutical interventions taken was 2.2. ICC significance scores were correlated with the pharmacist’s scores, ICC for consistency was 0.732 and 0.732 for absolute agreement, thus both can be considered as “good”. Potential for cost reduction associated with the recommended pharmaceutical changes, namely with medication being stopped or dose reduction was 32.7% (180/550) and 25.1% (138/550), respectively.
What next?
There is great potential and a definite need for the expansion of CPS in Austria. Only 15.8% of Austrian hospitals have a pharmacy department with even less offering CPS. Many countries have demonstrated the benefits of CPS in hospitals over the past 30 and more years. The need for increased pharmacist staffing in Austrian hospitals needs to be demonstrated to Austrian stakeholders.
Preparing for disaster – ensuring and optimizing the supply of medicines to a regional acute Hospital in the event of a major accident
European Statement
Patient Safety and Quality Assurance
Author(s)
Fabrizia Negrini, Giorgia Vella
Why was it done?
The aims of this project were firstly to optimize the content of the stock (choice of medicines and quantity) so that it is suitable for various potential events of different nature that may occur in the region. The second aim was to optimize the management processes in order to reduce costs.
What was done?
To manage extraordinary events (short-lasting phenomenon without contamination) in a region with 1.5 million inhabitants, the hospital pharmacy, in collaboration with a major acute Hospital, manages a designated stock containing medication that may be required during unplanned emergencies.
How was it done?
To achieve these two aims, the first step was to define which major events are possible and most likely to occur in the region. To do this we utilized a risk-based analysis of all disasters and emergencies relevant in the area that was performed by an external company that specializes in developing risk management projects in the context of civil protection1. Based on the identified events, we determined which types of injuries were more likely to occur. The medicine stock was subsequently updated and a process for minimizing the management cost was defined.
What has been achieved?
The hazards that were identified as being of particular importance for the analyzed region are likely to mainly result in blunt, perforating, and burn injuries. In collaboration with the Hospital, a list of 61 different medicines used to treat these types of injuries was established. In order to reduce costs, only drugs which were part of the main stock of the pharmacy were chosen. In this way, it is possible to exchange products with a longer shelf life from the main stock 6 months before expiring and use them without having to discard them.
What next?
In case of extraordinary events in a restricted region, the major acute hospital has an increased need for certain medicines. It is task of the hospital pharmacy to always be ready to supply them with such medicines. This is only possible if the probable emergency scenarios are well understood, and the stock and management processes are well-defined and communicated at all levels.
An interprofessional team for the management of nausea and vomiting in a haematological oncology unit
European Statement
Clinical Pharmacy Services
Author(s)
Mapi Fleury, Januska De Maria-Lee, Alessandra Taiana, Yvan Bourgeois, Sophie Voruz, Olivier Spertini, Pierre-Yves Bochud
Why was it done?
In 2019, procedural changes within unit treating malignant haemopathies raised awareness about unsatisfactory management of NV, particularly CINV. We identified a lack of departmental consensus, leading to heterogeneous therapeutic practices, confusion over the aetiologies of NV and feelings of powerlessness among healthcare professionals. We decided to improve the whole process, from prophylaxis to treatment, by addressing specific knowledge gaps concerning CINV, improving pathophysiological and pharmacological knowledge, and implementing interprofessional management and MASCC/ESMO guidelines.
What was done?
Patient nausea and vomiting (NV)—particularly chemotherapy-induced NV (CINV) in malignant haemopathies—was managed by an interprofessional team.
How was it done?
A multidisciplinary working group was established to create a comprehensive, patient-centred NV management programme. Work sessions focussed on attaining a therapeutic consensus and adapting international guidelines to our context. Different professions learnt about each other’s needs and fields of competency, enabling each to be heard and creating mutual benefits through sharing expertise and knowledge. Pathophysiological/pharmacological leadership was given to clinical pharmacist, including developing and teaching specific protocols and supervising complex clinical situations in the field.
What has been achieved?
Interprofessional consensus was reached, documentation and techniques were implemented including clinical evaluation checklists at patient admission. CINV therapeutic regimens were completely updated and immediately and automatically included in cancer treatment protocols. The clinical pharmacist and specialist nurses give initial interprofessional training to new colleagues and ensure continuous on-site supervision. This transversal work has resulted in fewer patients suffering from NV and better team understanding of pathophysiological mechanisms, differential diagnoses and adverse drug effects—this also ended the use of unsuitable medications and dosages. Overcoming this critical situation also allowed us to begin non-pharmacological integrative care.
What next?
Interprofessional working group proved indispensable to this approach. Including CINV pharmacotherapy directly into cancer treatment plans is one of programme’s strong points and contributes to high adherence to guidelines. Team feels more relaxed and more in control. Monitoring is now done by tracking files and oral feedback, but we aim to implement systematic follow-up of interventions, care evaluations and NV to assess programme’s impact. Next stage will also include patient feedback.
OPTIMIZATION AND CENTRALIZATION OF THE HANDLING CIRCUIT OF HAZARD DRUGS FROM THE PHARMACY SERVICE
European Statement
Clinical Pharmacy Services
Author(s)
Mireia Iglesias Rodrigo, Júlia Pardo Pastor, Alba Manzaneque Gordon, Cristina Sangrador Pelluz, Núria Meca Casasnovas, Clara Sebastián Carrasco, Fernando Salazar Gonzalez, Gemma Garreta Fontelles, Jordi Nicolás Picó
Why was it done?
Due to the risk posed by the handling of Hazard Drugs (HD) in the healthcare field, it is necessary to implement circuits that guarantee the professional’s safety.
What was done?
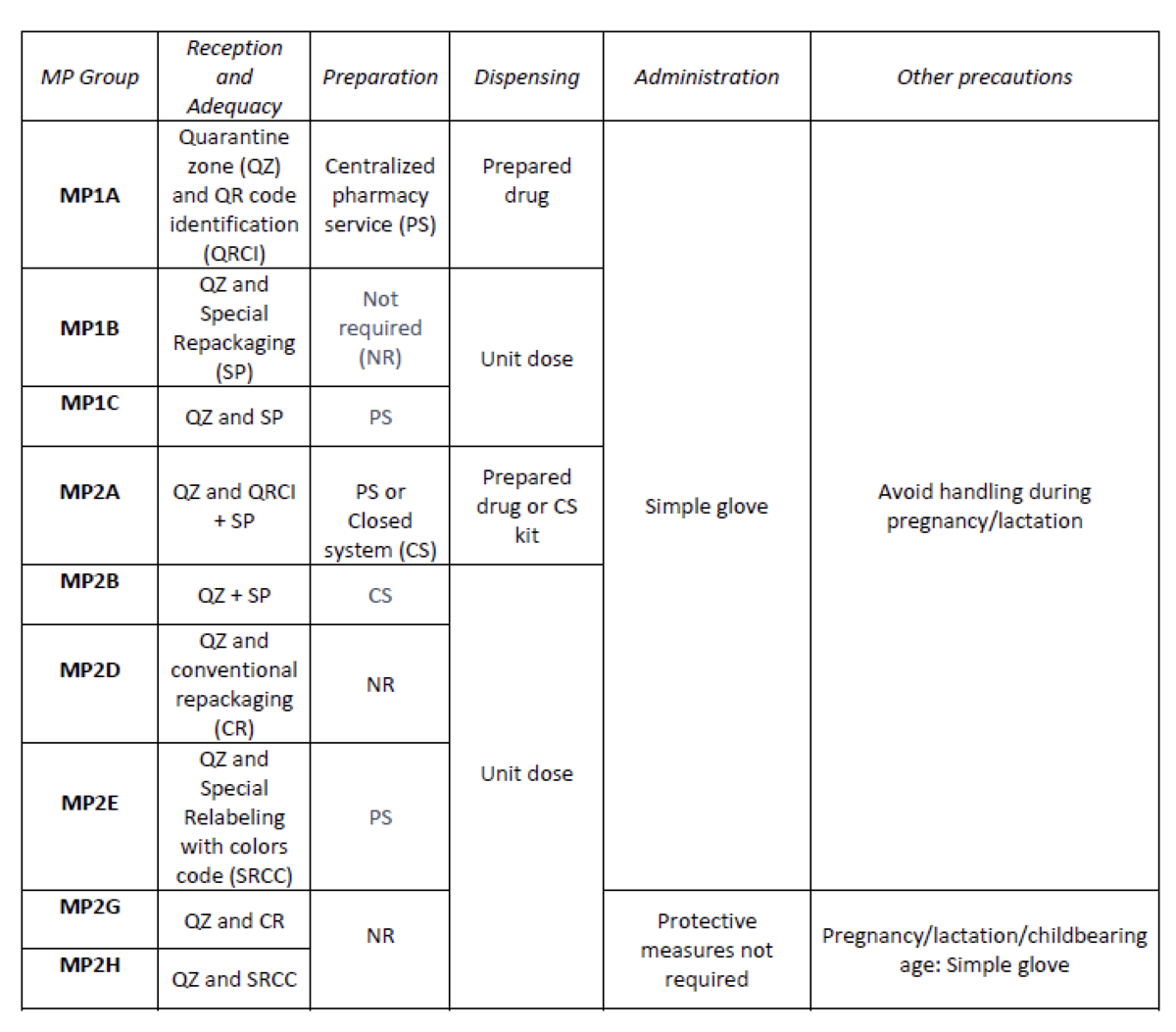
Create an internal classification of HD based on the NIOSH List of Hazard Drugs in Healthcare Setting 2020, to optimize the circuit of its handling from its receiving to its administration.
How was it done?
Considering the HD included in the Pharmacotherapeutic Guide (PTG) of our center, the stages of reception and adaptation/preparation/dispensing/administration and other precautions were analyzed.
Categories were established, analyzing the needs of each stage according to: NIOSH level of danger, setting (inpatient/outpatient), pharmaceutical form, commercialized pharmaceutical specialties or available alternatives, and material/personal resources.
Prior to its implementation, e-learning training was carried out for the healthcare professional involved.
What has been achieved?
A total of 25.3% (379/1498) of the pharmaceutical specialties included in PTG were HD. Thirteen HD groups were identified. Due to the fact that in the outpatient setting the drug is dispensed to the patient in its original container, the actions implemented were only carried out for inpatients, representing these 9/13 of described groups. The established training was carried out by the 89% of professionals. Proposed measures for HD are summarized in Table 1.
What next?
Monitoring and evaluation of the circuit
Optimizing information on the fecal microbiota transplantation circuit
European Statement
Patient Safety and Quality Assurance
Author(s)
Julia Santucci, Céline Vaesken, Guillaume Saint-Lorant
Why was it done?
FMT is a therapy introduced in 2016 at the hospital. It is indicated for the management of recurrent and refractory Clostridioides difficile (CD) infections. In November 2020, with the resumption of the activity, we note a lack of knowledge of the different actors on this circuit: physician, nurses, fellows, patients himself.
The objective of the study is to reinforce the understanding and safety of the FMT circuit in a university hospital after the evaluation of the knowledge of the different actors.
What was done?
Implementation of a document to represent the circuit of fecal microbiota transplantation (FMT) in a French university hospital.
How was it done?
In this context, two questionnaires containing less than five questions on the functioning of the circuit were carried out with the nurse coordinators (NC) and the interns of the hepato-gastrology department. Subsequently, a document was drafted in consultation with the referring physician, the head of department and the pharmaceutical team to represent the FMT circuit.
What has been achieved?
With regard to the questionnaires, we obtained six answers from the NC, with 42% correct answers, 25% partial answers and 33% incorrect answers, and then six answers from the residents, with 20% correct answers, 7% partial answers and 77% incorrect answers.
These questions made it possible to draw up a diagram adapted to A4 format intended for all the actors in the circuit. It defines the different missions of all the actors with the corresponding deadlines and associated procedures.
In order to improve information, two interventions were carried out by the pharmacy: a staff meeting dedicated to the management of CD infections with the interns, co-hosted with the referring physician, and a presentation of the circuit to the NC.
What next?
Finally, this study made it possible to reinforce the safety of the FMT activity for the patient and to improve the management of the circuit for the various health professionals involved in this specialized therapy.
Implementation of a workshop about the role of the hospital pharmacist role during the clinical clerkship in medical training
European Statement
Education and Research
Author(s)
Vincent ARCANI, Stéphane HONORÉ, Guillaume HACHE
Why was it done?
Interprofessional collaboration as an effective means for improving healthcare outcomes. In order to achieve an effective level of collaborative healthcare practice, health care educators must focus attention on interprofessional education in undergraduate programs. Knowledge of professional role of others is a key competency for interprofessional practices and there is a lack of knowledge on hospital pharmacists’ roles among other health care professionals.
What was done?
We developed a workshop focused on the role of hospital pharmacists, to be integrated into the curricula of other health professionals.
How was it done?
The workshop was developed by a resident in hospital pharmacy and a senior hospital pharmacist, and we first targeted medical curriculum. The session integrated: students’ perception of hospital pharmacists’ role, didactic learning on the role of hospital pharmacists according to the European statements in hospital pharmacy, immersion in practice and evaluation. The assessment of the learning effect was performed by a pre-/post-workshop questionnaire, assessing satisfaction, metacognition and acquired knowledge. In addition, students provided open feedback on the workshop.
What has been achieved?
We implemented the workshop during the first year of clinical clerkship in medical education. Preliminary results highlighted (i) a high satisfaction, illustrating the relevance of the initiative; (ii) an increase in perceived knowledge and (iii) an increase in knowledge about hospital pharmacists’ roles, especially about pharmaceutical technologies and medical devices. Verbatim analysis of the feedback suggested that the workshop modified medical students’ perceptions on the role of hospital pharmacists, and that they may be more inclined to seek collaboration with hospital pharmacists.
What next?
To integrate the workshop into the curricula of the other professions in order to raise awareness on hospital pharmacy and promote interprofessional teamwork.